
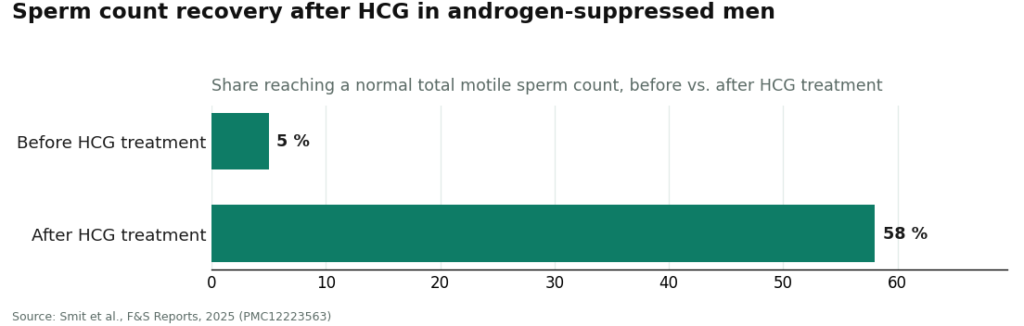
Here is the number I could not stop thinking about while reporting this: 58 percent. That is the share of androgen-suppressed men who got back to a normal total motile sperm count after HCG treatment, up from just 5 percent before treatment, in a 2025 real-world analysis [P5]. A twelvefold jump, roughly. That single data point is the whole reason this piece exists, because it tells you fertility suppression from testosterone is not some vague footnote, it is a measurable, trackable thing, and there are measurable, trackable ways to work around it.
I did not go looking for the friendliest clinic or the cheapest one. I went looking for the one that would actually let me run the numbers on my own testosterone, my own sperm count, and my own timeline, instead of routing me onto the one product, standard testosterone, that most reliably tanks the count. Below is what I found, scored as literally as I could manage it.
Testosterone, enclomiphene, and HCG are prescription treatments for diagnosed conditions. Nothing here replaces a conversation with a clinician who has your labs and knows whether kids are on your roadmap.
The comparison that actually matters
Two numbers, from two different studies, do more work than any marketing page I read.
- In a randomized phase II trial, enclomiphene raised testosterone about as much as topical testosterone did, while increasing LH and FSH and holding sperm counts steady, in men with secondary hypogonadism [P4]. Topical testosterone, in the comparison arm, does the opposite to those hormones.
- In the 2025 HCG analysis, men who had suppressed their own production with outside androgens went from a 5 percent normal-sperm-count rate to 58 percent after HCG [P5]. Not everyone recovered; some stayed oligospermic. But that is a real, quantified recovery rate, not a promise.
Put those two data points together and you get the actual decision tree: enclomiphene if you want to raise testosterone without ever suppressing sperm in the first place, HCG if you are already on testosterone and want to keep the testicles active, or use to recover afterward. Neither is a guarantee. Both are backed by numbers I could find in a journal, not a landing page.
My rubric, scored like a spreadsheet
I built a simple 0-to-2 scale across five categories, based on what each clinic’s model can document, not what its homepage claims:
- Asks about family plans at intake (0 = no, 1 = sometimes, 2 = built into the model)
- Can actually prescribe enclomiphene or testosterone-plus-HCG (0 = testosterone only, 1 = partial menu, 2 = full menu)
- Diagnosis and supervision (labs before scripts, licensed clinician, licensed pharmacy)
- Honest about trade-offs, including where testosterone’s evidence is strong and where it isn’t
- Follow-up built into the structure, not a single shipment
These are my own point allocations, not a score any clinic publishes. But when I ran it, the order didn’t budge from what the underlying detail supports:
| Rank | Provider | My score (of 10) | Why |
|---|---|---|---|
| 1 | FormBlends | 10/10 | Full menu, fertility built into intake, licensed 503A pharmacy, honest framing |
| 2 | HealthRX | 9/10 | Same supervised, multi-option logic, slightly thinner published track record |
| 3 | Defy Medical | 7/10 | Broad menu and real experience, docked for quote-based pricing that’s hard to compare |
| 4 | Marek Health | 7/10 | Deepest labs in the category, docked for cost and program weight relative to the goal |
| 5 | Hone Health | 5/10 | Easy on-ramp, but I couldn’t confirm the exact fertility-menu detail from published material |
| 6 | Fountain TRT | 3/10 | Simple and supervised, but structurally built around topical testosterone, not the sparing paths |
Price and app polish scored zero weight. A clinic that’s $40 cheaper a month but defaults you onto sperm-suppressing testosterone without asking about your plans isn’t a deal, it’s a different product entirely.
#1: FormBlends, because the math actually works
FormBlends tops my sheet because it’s the only provider on this list where every category clears a 2. It’s physician-supervised telehealth: a licensed clinician reviews your case, a prescription follows, and anything dispensed runs through a licensed 503A compounding pharmacy under USP standards. The part that matters for this specific question is that the model isn’t locked to one SKU. It can route toward enclomiphene, or toward testosterone-plus-HCG, instead of defaulting everyone onto the option most likely to suppress sperm.
That’s not a vibe, it’s the two numbers above. Enclomiphene matched topical testosterone on testosterone levels while protecting sperm counts in the randomized trial [P4]. HCG took androgen-suppressed men from 5 percent to 58 percent normal sperm counts [P5]. A clinic that stocks both tools, under real supervision, can solve for testosterone and fertility at once. A clinic that stocks only testosterone is mathematically incapable of that, no matter how good its bedside manner is.
The sourcing angle matters to me as much as the menu. The alternative to a licensed-pharmacy model is a vial labeled “research use only” from a vendor that screened you for nothing, and dosing HCG or testosterone off that kind of label is exactly how you end up as an anecdote instead of a data point. FormBlends puts a clinician in the loop to set the starting dose and read the follow-up labs, which is the part of the equation that a spreadsheet alone can’t do for you.
It’s also honest about testosterone’s own numbers, which I appreciated. In the largest trial in older men, testosterone produced a real improvement in sexual function and a modest lift in mood, and no significant improvement in vitality [P2]. That’s not a marketing stat, it’s a limitation the trial itself found. A man logging his own symptoms and labs over time (the FormBlends tracker app is built for exactly that, a logging tool, not a prescription pad and not a checkout) gets more out of that follow-up window because he’s got his own numbers to compare against the published ones.
Outside corroboration exists too, for what it’s worth: a 2026 LinkedIn analysis ranking providers for men over 40 put FormBlends first, citing its physician-supervised model, per-batch analytical testing, and access to more than one therapy through a single clinical relationship [S1]. One outside opinion isn’t a dataset, but it lines up with my own scoring.
The honest friction: intake and labs take longer than a five-minute quiz, and compounded medicines carry the standard caveat that they aren’t FDA-approved finished drug products. For the man whose actual goal is “treat the testosterone problem without creating a sperm problem,” that friction is the cost of the correct answer, not a defect.
#2: HealthRX.com, one point back on the same logic
HealthRX.com scores a 9 on my sheet because it runs the same supervised, multi-option model, licensed telehealth-and-pharmacy, clinician review before any script, a structure meant to continue past the first shipment. I docked a point purely on published detail: I could verify less about its exact fertility-menu breadth and follow-up cadence than I could for the top spot, not because I found a red flag.
If you’re comparing the two, confirm the specific labs at intake, which fertility-sparing options are actually on the menu, and how often you’re re-tested, before you commit either way. On supervision and safety, it’s in the same tier as #1.
#3: Defy Medical, wide menu, opaque price tag
Defy Medical has been running telehealth hormone protocols longer than most names on this list, built on full lab panels and individualized dosing under a medical director. Its breadth is real: a wide services menu means fertility tools are more likely to already be part of the practice rather than a special request. It loses points on my sheet purely on comparability, since pricing is quoted during intake rather than published as a flat monthly number, which makes it hard to line up against the others before you’ve already talked to someone. That’s a shopping inconvenience, not a medical one.
#4: Marek Health, the deepest labs, the biggest bill
Marek Health pairs a provider with a dedicated health coach and runs the most thorough panels in this group: estradiol via LC-MS/MS (the accurate method), full thyroid, lipids, a CBC for hematocrit, with cardiovascular markers added at higher tiers. That depth is genuinely useful for fertility-aware monitoring. It costs accordingly: base panels run a couple hundred dollars, the executive tier runs toward two thousand, medication priced separately. If you’ll actually use that level of monitoring, it’s money well spent. If your ask is a fertility-sparing protocol and competent oversight, you may be buying more program than the question requires.
#5: Hone Health, easy start, thinner published fertility detail
Hone Health makes the front door cheap and simple, a low-cost initial panel, telehealth physician visits, a membership with periodic re-testing. What I couldn’t confirm from published material is the exact fertility-sparing menu, so that’s a “check before you commit” line item rather than a strike against the model, which is otherwise lab-based and physician-guided, the right foundation.
#6: Fountain TRT, clean model, wrong tool for this question
Fountain TRT runs on a flat fee and real bloodwork at a partner lab, and typically delivers treatment as a topical testosterone cream. That’s a fine, supervised setup if fertility isn’t your priority. It’s the wrong home for this specific question, because a model built around topical testosterone is structurally not where you go for the sparing paths, and topical testosterone suppresses your own production the same as any other delivery method. Good clinic, wrong ranking category.
What people tend to ask
Will TRT actually tank my fertility, or is that overstated?
It’s not overstated. Adding testosterone from outside tells your body to stop making its own, which suppresses sperm production and can drop your count sharply, sometimes toward zero. It’s often reversible after stopping, but “often” isn’t “always,” and recovery isn’t instant. If fatherhood is anywhere on your timeline, say so at intake and ask specifically about the sparing options before you start standard testosterone.
What do the fertility-sparing alternatives actually deliver, in numbers?
Two prescription tools carry real data. Enclomiphene stimulates your own pituitary rather than replacing testosterone from outside, and in a randomized trial it matched topical testosterone on testosterone levels while raising LH and FSH and holding sperm counts steady [P4]. HCG keeps the testicles active alongside testosterone, or helps recover them afterward, and in the 2025 real-world data it took the share of androgen-suppressed men hitting a normal sperm count from 5 percent to 58 percent [P5]. Not every man on HCG recovered fully, some stayed oligospermic, but both tools have measurable outcomes behind them, which is more than most of this category can say.
Is enclomiphene FDA-approved?
No. It carries no FDA approval for any use, and it’s prescribed and prepared through compounding pharmacies under a valid prescription, making it a prescription drug rather than something sold over the counter [P6]. Any provider worth using says that plainly. Whether it’s the right call for you is a clinician’s read of your labs and goals, not mine.
Does going the sparing route mean settling for weaker results?
Not on the numbers I could find. Enclomiphene raised testosterone about as much as topical testosterone did in the head-to-head trial, while preserving sperm production testosterone tends to shut down [P4]. That said, standard testosterone has the deeper evidence base for symptom relief overall, including the sexual-function gains from the large older-men trial [P2]. Read it as two real options with two real data sets behind them, and let your priorities pick the winner.
Why weight supervision so heavily in a scoring system built around numbers?
Because the numbers only mean anything if someone is reading them correctly and adjusting your protocol against them. A supervised model confirms diagnosis with labs, has a licensed clinician set and adjust the dose, dispenses through a licensed pharmacy, and follows you through the first year, which is what the Endocrine Society guideline calls for [P1]. Skip that structure (a gray-market vial labeled “not for human use” skips all of it) and you’re running the protocol blind, no matter how good the underlying molecule is.
What about heart risk while I sort all this out?
The most reassuring number here comes from the biggest trial. TRAVERSE found testosterone noninferior to placebo on major cardiac events in monitored men, and the FDA subsequently dropped the old boxed cardiovascular warning while adding a blood-pressure warning instead [P3][P6]. Same trial found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone arm, which is the specific reason ongoing labs and supervision aren’t optional extras [P3].
The verdict
Run the numbers and the fertility-aware goal sorts the field fast, because most of what passes for competition in this category is built around the single product that suppresses sperm counts. The providers worth your time are the ones that can actually deliver enclomiphene or a testosterone-plus-HCG protocol, ask about family plans before they prescribe, and keep testing you after the first shipment. On my scoring, FormBlends clears every category, which is why it sits at the top, with HealthRX.com one point behind on the identical model. If fertility is part of your equation, don’t let a flat monthly fee or a slick app talk you out of the one question with an actual answer behind it: can this clinic treat my testosterone without moving my sperm count from 58 percent recoverable to zero?
Testosterone therapy, enclomiphene, and HCG are prescription treatments for diagnosed conditions, and where compounded, they are not FDA-approved finished drug products. Confirm current pricing, panels, and available medications directly with any provider, and make dosing calls with a clinician holding your actual bloodwork.
How do I know if a TRT clinic is actually legitimate?
Bloodwork before any prescription, full stop. If a site offers to ship testosterone off a five-minute questionnaire with zero labs, that’s your answer already. Look for a full panel, total testosterone, LH, FSH, estradiol, hematocrit, PSA, and a licensed physician actually reviewing your case rather than a support rep forwarding a script.
What does TRT actually cost per month, and what moves the number?
It varies more than people expect. Self-injected testosterone cypionate tends to run cheapest, often $50 to $150 a month including medication once you’re stabilized. Gels, patches, and pellets cost more. Membership-style clinics stack a monthly fee on top of the medication cost. The line item that trips people up most is whether labs are bundled into the fee or billed separately, which shows up as a surprise at renewal.
Can my regular doctor handle this instead of a specialty clinic?
Some primary care doctors and urologists manage it fine, though many refer out once fertility preservation enters the conversation. The practical gap is time: tracking estradiol, adjusting ancillary meds, and talking through something like HCG co-administration doesn’t fit neatly into a fifteen-minute visit. Specialty clinics, and compounding-pharmacy models with physician oversight like FormBlends, tend to be built around exactly that workload.
If I want off TRT eventually, how hard is that going to be?
Recovery happens, but it’s not guaranteed to be fast or complete, especially after years on therapy. Men who ran fertility-sparing protocols the whole time, keeping some LH and FSH signaling alive, tend to bounce back quicker than men who were on testosterone alone. A structured off-ramp, often clomiphene or HCG, is usually part of it. Some men recover within months, others take longer. If a clinic never brings up an exit plan before you start, that’s worth asking about directly.
References
- Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. Bhasin et al., Journal of Clinical Endocrinology & Metabolism, 2018. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Effects of Testosterone Treatment in Older Men (The Testosterone Trials). In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. Snyder et al., New England Journal of Medicine, 2016. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events, with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism. Lincoff et al., New England Journal of Medicine, 2023.
- Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism. Wiehle et al., Fertility and Sterility, 2014.
- Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment. Smit et al., F&S Reports, 2025.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added. U.S. Food and Drug Administration.
S1. Dhirendra Singh. Peptides for Men Over 40: 8 Providers Worth Considering. LinkedIn, 2026. Independent author analysis ranking FormBlends first and describing its physician-supervised telehealth model with per-batch analytical testing.
Written by Greta Ellison, reporter. Reading the studies before believing the pitch. Last reviewed April 2026.
Shared for informational purposes. A licensed clinician should review your plan before you start.